Acute Stroke Unit care
People with acute onset of aphasia should be suspected of having a stroke and transferred directly to a hospital with an acute stroke unit and admitted to the acute stroke unit.
Reference: Stroke Unit Trialists, 2007
NHMRC Level of Evidence: I
Rationale: There is strong evidence that patients who receive organised stroke unit care are more likely to survive their stroke, return home and make a good recovery (Stroke Unit Trialists, 2007).
Acute Stroke Unit care
Stroke unit care has some of the strongest evidence for improved patient outcomes in the stroke research literature. Patients who receive organised stroke unit care are more likely to survive their stroke, return home and make a good recovery (Stroke Unit Trialists Collaboration, 2007).
As such, the National Stroke Foundation (NSF) recommends that all people with stroke be admitted to hospital and treated in a stroke unit with a multidisciplinary team (National Stroke Foundation, 2010). This evidence can be used to advocate for the best treatment for people with aphasia, including transfers to a stroke unit if necessary.
People with aphasia are at a higher risk of not receiving stroke unit care. Engelter et al. (2006) reports that cardiac embolisms are associated with an increased risk of aphasia. As such, people with aphasia are more likely to end up on cardiac wards rather than receiving stroke unit care.
Distinctive features of a stroke unit as defined by the Stroke Unit Trialists’ Collaboration (2007) are:
- Coordinated multidisciplinary team care
- Staff with special interest in stroke
- Routine involvement of caregivers
- Continued education and training programs
Studies have continued to show the benefit of dedicated stroke care since 1980. An initial study by Garraway et al (1980) showed significant improvement in stroke survival and recovery rates in those treated in stroke units as compared to medical units.
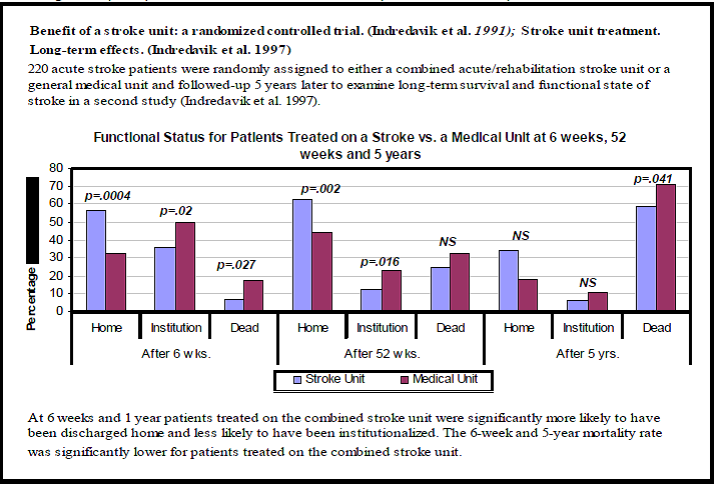
The Stroke Unit Trialists’ Collaboration (2007) provides the largest systematic review of organised inpatient stroke units compared to less-organised conventional care. Stroke unit care was shown to reduce the likelihood of death and disability and stroke severity by as much as 30% at final 1 year follow-up. Similar results have also been seen in a systematic review of observational studies of stroke unit implementation (Seenan et al., 2007), evidence that the benefit of stroke units translates across into trials more closely approximated with usual care. Studies such as that by Indredavik et al. (1991) have also shown improvement in long-term survival (after 5 years) in patients treated in a stroke unit as compared to a medical unit (see Figure 2).
RESOURCE:
Where can I find more information about stroke units in Australia?
- The National Stroke Foundation provides a list of acute stroke units in Australia.
References:
- National Stroke Foundation. (2010). Clinical guidelines of stroke management 2010, Melbourne, Australia
- Stroke Unit Trialists, C. (2007) "Organised inpatient (stroke unit) care for stroke." Cochrane Database of Systematic Reviews DOI: 10.1002/14651858.CD000197.pub2.
- Engelter, Stefan T., et al. "Epidemiology of aphasia attributable to first ischemic stroke incidence, severity, fluency, etiology, and thrombolysis."Stroke 37.6 (2006): 1379-1384.
- Garraway, W. M., Akhtar, A. J., Prescott, R. J., & Hockey, L. (1980). Management of acute stroke in the elderly: preliminary results of a controlled trial. Br Med J, 280(6220), 1040-1043.
- Seenan, P., Long, M., & Langhorne, P. (2007). Stroke units in their natural habitat: systematic review of observational studies. Stroke, 38(6), 1886-1892. doi: 10.1161/STROKEAHA.106.480871
- Indredavik, B., Bakke, F., Solberg, R., Rokseth, R., Haaheim, L. L., & Holme, I. (1991). Benefit of a stroke unit: a randomized controlled trial. Stroke, 22(8), 1026-1031. doi: 10.1161/01.str.22.8.1026
GET IN TOUCH
l.worrall@uq.edu.au | |
+61 7 3365 2891 | |
Professor Linda Worrall |
RESEARCH PARTNERS






